One Step Closer to Treating Children with Bell’s Palsy

Bell’s Palsy causes a sudden weakness on one side of the face affecting roughly 6–19 children per 100 000 per year. The symptoms have rapid onset and include disordered movement of facial muscles/loss of sensation, headaches, tearing, drooling, loss of taste and hypersensitivity to sound (Fig.1).
While the exact cause is unknown, studies have suggested that viral infections and inflammation as two potential contributors. Existing treatments for adults with Bell’s Palsy include the use of corticosteroids to counteract the inflammation and/or antiviral treatment to target latent viruses. In addition to this, other treatments like botulinum toxin, physiotherapy, hyperbaric oxygen (i.e. giving the body extra oxygen), acupuncture and surgery have also been explored in adults. However, the use of these treatments and the most effective treatment in children aged under 18 remains uncertain.
")
What are we solving for?
Through my research component with Dr. Frank Sullivan, I am part of a team undertaking a Cochrane collaboration review of the medical management of Bell’s Palsy. I am involved with a sub-group analysis to answer the question “How should children with Bell’s Palsy be treated?”. I’ve learned that a systematic review is often the gold standard in medical research because it involves identifying, appraising, and synthesizing the empirical evidence from multiple studies to arrive at a reliable conclusion (Fig.2). Our systematic review will aim to include recent clinical trials data from the BellPIC study in Australian pediatric units, compare all available medical treatments and provide a comprehensive and up to date overview on this topic.
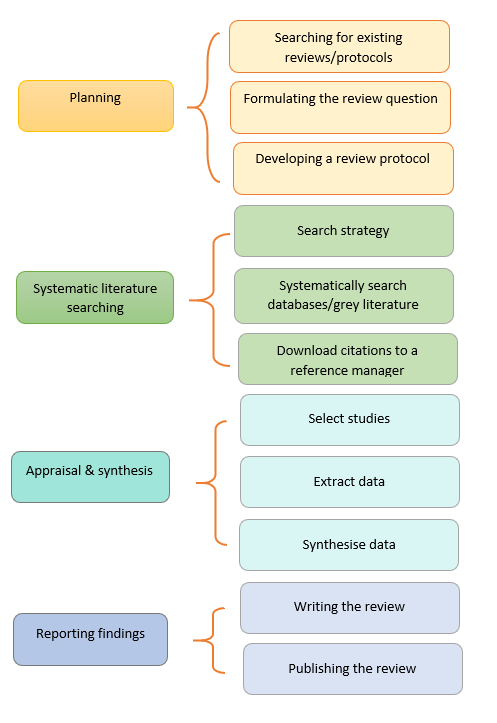
Figure 2. Steps involved in a systematic review (AUT Library ©)
Impact and why does it matter?
If left untreated, Bell’s Palsy can sometimes lead to extensive functional impairment and disfigurement of the face as well affect mental health and diminish quality of life in children.
As such, a lack of up-to-date systematic reviews can compromise medical treatment, increase patient's anxiety, cause a waste of time and money, and result in prolonged disability, it is hoped that the results of this review will provide some reassurance and clarity to both doctors and patients in the management of children's Bell’s Palsy.
My Laidlaw experience so far:
I’m collaborating with researchers in St Andrews and Australia to develop my skills in study design, identifying relevant studies, assessing bias and quality of studies, summarizing evidence and interpreting findings. A typical day involves completing modules on how to undertake a systematic review, carrying out literature searches for studies in children, contacting study authors to request more information, extracting study details and meeting with professors and primary care physicians to resolve by consensus any discrepancies regarding the extracted data. Furthermore, I was also actively involved in writing the study protocol which has been submitted to Cochrane review. Due to the timing of the project and awaiting to hear from the journal, it hasn’t been possible to extract data from as many studies as I would’ve liked to over my 6 week research period. I recall telling myself “It’s ok for plans to change” and reminding myself to adapt to each situation as they arise. As a possible solution, I requested my supervisor that I continue to be involved in the project even past the 6-week timeline. This would let me assess and include more studies once they come through from Cochrane, and arrive at a more comprehensive review. I was very pleased that my supervisor was so open to the idea!
It was my first time undertaking a systematic review so I did face some other roadblocks too. For instance, these ranged from trying to figure out how to better grasp minor details from scientific papers or trying to manage my time more effectively whilst working remotely. Fortunately, the talks and socials hosted by Laidlaw helped us talk through some of the challenges we were facing. This was especially reflected through the Action Learning Sets (ALS) where we actively helped each other through some of these issues and offered advice or support to other scholars. It was also a nice reminder of the things we were all doing right!
What’s next?
We’re still awaiting to hear from Cochrane review about the studies we can include in our analysis. Following this, we will further extract data from studies, carefully assess for bias and strength of each study and try to identify what the best course of treatment is for children with Bell’s Palsy.
My 3 Key takeaways:
It’s ok to ask for help.
It’s ok for plans to change.
It’s ok to say “good job” when you get something right.
I am very grateful to the Laidlaw Scholars Program and everyone involved in providing us with the educational and enriching experience of a lifetime!
References:
Copp F. The Droopy Dribbler: Paediatric Presentations of Bell’s Palsy. RCEM Learning. 2020 May. Available at: https://www.rcemlearning.co.uk/foamed/the-droopy-dribbler-paediatric-presentations-of-bells-palsy/.
Hogg ES, Hampton T, Street I, Clarke R, Wright K, De S, Sharma SD. Increased incidence of idiopathic paediatric facial palsy during the coronavirus disease 2019 pandemic. J Laryngol Otol. 2021 Aug;135(8):668-670. doi: 10.1017/S0022215121001353. Epub 2021 May 12. PMID: 33975658; PMCID: PMC8245328.
Jalali MM, Soleimani R, Soltanipour S, Jalali SM. Pharmacological Treatments of Bell's Palsy in Adults: A Systematic Review and Network Meta-Analysis. Laryngoscope. 2021 Jul;131(7):1615-1625. doi: 10.1002/lary.29368. Epub 2021 Jan 6. PMID: 33404068.
Somasundara D, Sullivan F. Management of Bell's palsy. Aust Prescr. 2017 Jun;40(3):94-97. doi: 10.18773/austprescr.2017.030. Epub 2017 Jun 1. PMID: 28798513; PMCID: PMC5478391.





Please sign in
If you are a registered user on Laidlaw Scholars Network, please sign in